

- Who We Are
- DIMES
- Our Products
- Amorphous hydrogel Dressing
- Sliver Wound Gel
- PHMB Antibacterial Alginate Dressing
- Silver Alginate Dressing
- Extra Silver Alginate Dressing
- Extra Silver Gelling Fiber Dressing
- Silver Gelling Fiber Surgical Dressing
- Silver PU Antibacterial Foam Dressing
- Silicone Ag Foam Dressing
- Alginate Dressing
- Silicone Postoperative Dressing
- Foam Dressing
- Medical Hydrogel Dressing
- Silicone Foam Dressing
- Silicone Foam Dressing Border Yoga
- Super Absorbent Dressing
- Gelling Fiber Dressing
- Collagen Wound Dressing
- Collagen Particles
- Silicone Tape
- Silicone Gel Scar Dressing
- Silicone Wound Contact Dressing
- Tech Services
Silver Sustained Release Antibacterial Technology

OptiSil Silicone Perforation Technology

Absorption and Degradation Metabolism Technology

Anti-adhesion Technology
- Blog
- Contact Us
- Case Study
Amorphous Hydrogel Dressing
Trauma Right Anterior Tibia (Case 18)
This is a 54 y/o male with hx of a motorcycle accident which resulted in a right grade 3 open bicondylar tibial plateau fracture. He is s/p external fixation with a subsequent reduction internal fixation. Upon presentation the anterior tibial wound, which occurred during the accident, had been open for 3 months. His surgical incisions were closed. Pt was placed on NPWT x 3 weeks then transferred to PHMB alginate dressings on week 4. Pt was also treated with weekly ultrasonic debridements. Double Tubigrips™ were applied to the RLE. Wound closed 49 days after PHMB alginate was initiated.

Diabetic Foot Ulcer Right Foot (Case 19)
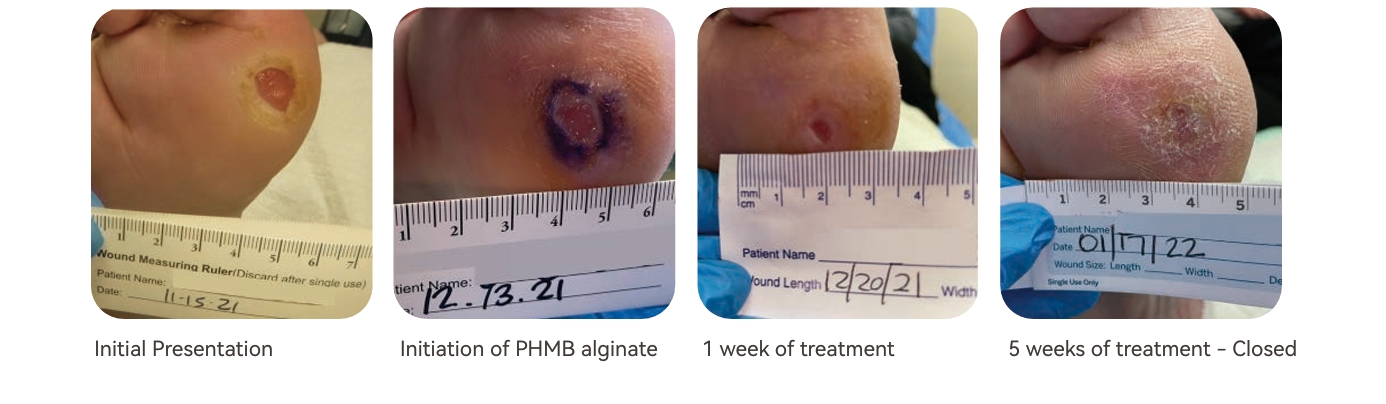
This is a 49 y/o female with hx of CHF, type 1 diabetes, obesity, BLE chronic DVTs, and previous left BKA due to osteomyelitis presented with a non-healing WG1 DFU to the right plantar first met head. Pt was off loading with a wheelchair due to her recent left BKA and was initiated on PHMB alginate with dressing changes 3 times weekly. She was treated with serial weekly ultrasonic debridements and PHMB alginate dressings and wound was closed in 35 days.
Diabetic Foot Ulcer Left Ankle (Case 20)
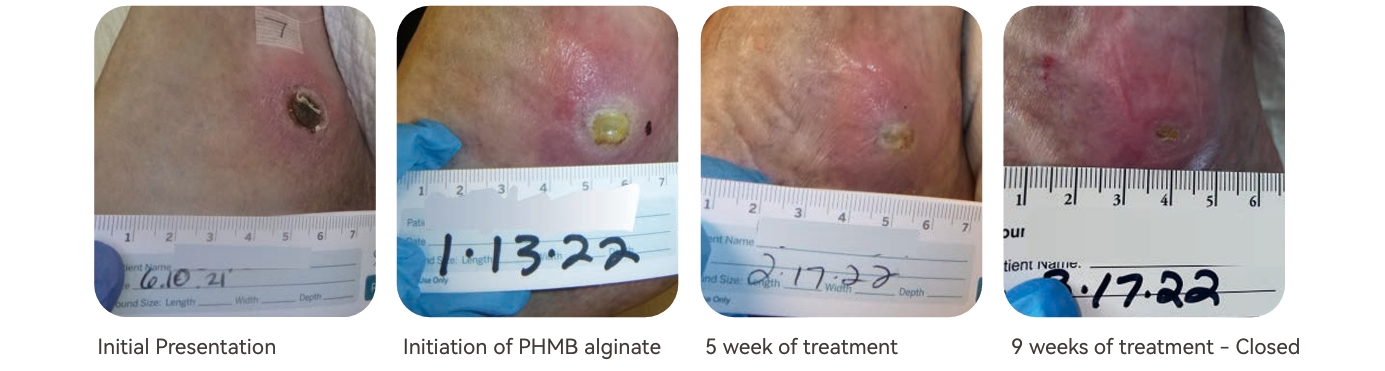
This is a 75 y/o male with hx of diabetes type 2 with neuropathy and severe psoriasis with a left lateral ankle wound which had been present for 7 months prior to PHMB alginate being initiated. Vascular status was verified and was adequate. MRI was negative for osteomyelitis. Wound culture was negative. PHMB alginate was started on week 31 of treatment. After 6 weeks of PHMB alginate treatments, triamcinolone 0.1% was started to periwound with dressing changes to aid in control of psoriasis related inflammation. Pt wound closed 64 days after PHMB alginate was initiated.
Venous Stasis Ulcer Left Leg (Case 21)
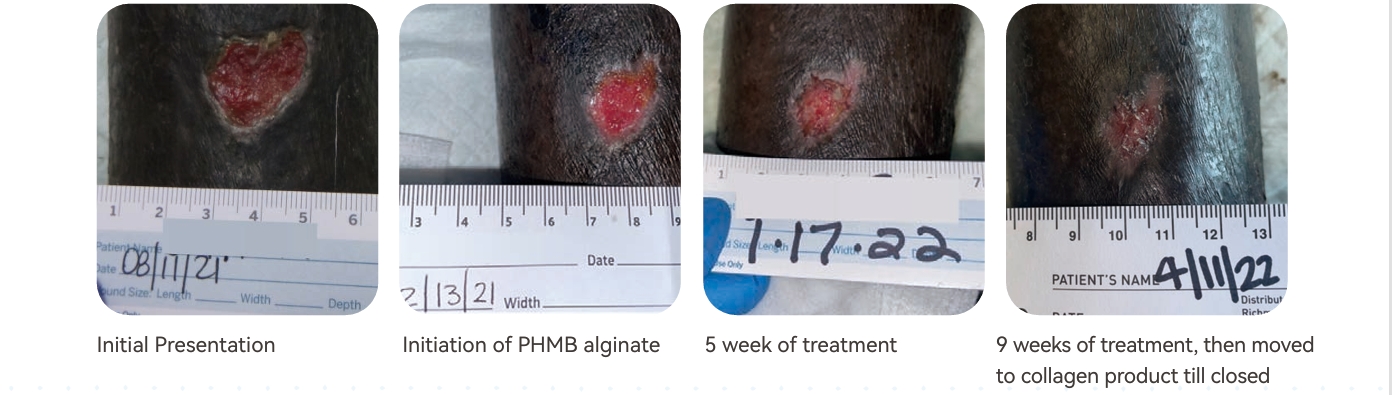
This is an 86 y/o male with hx of severe peripheral arterial disease as well as chronic DVT’s. Pt was revascularized and is s/p atherectomy with balloon angio of the left SFA and AT however arterial flow was unable to be fully restored. Pt was offered BKA and refused. PHMB alginate, weekly ultrasonic debridements, and a single tubi grip were initiated on week 18 of wound treatment and there was a 91% improvement in the area of the wound after 63 days of PHMB alginate. The patient was then transitioned to a collagen product to complete wound closure.
Results
In full thickness wounds, Alg/PHMB formed vascularized granulation tissue and resulted in improved epitheliali zation. These wounds included diabetic foot ulcers, trauma wounds, as well as arterial and venous leg ulcers. Patient co-morbidities included diabetes, obesity, psoriasis, and peripheral vascular disease. Average initial wound size ranged from 1 – 4 cm2. The number of Alg/PHMB applications ranged from 5 – 14 and time to com plete wound epithelialization ranged from 35 – 98 days. None of these patients developed wound infections during their course of treatment.
Conclusion
This case series demonstrates the successful treatment of complex wounds using adequate wound bed prepara tion and an alginate dressing containing 0.8% PHMB. The topical dressing was assimilated with surrounding viable tissue, preventing infection, building granulation tissue, and encouraging neoepithelialization in stalled, chronic wounds. Similar outcomes have been achieved with a porcine collagen matrix containing 0.1% PHMB for burns, venous ulcers, surgical wounds, and scar tissue. Further study is warranted to determine if Alg/PHMB can be a stand-alone dressing or possibly a cover dressing over skin substitutes to improve healing efficacy.
References
1. Butcher, M. (2012). PHMB: An e�ective antimicrobial in wound bioburden management. British Journal of Nursing, 21(Sup8). https://doi.org/10.12968/b jon.2012.21.sup8.s16
2. Gray, D., Barrett, S., Battacharyya, M., Butcher, M., Enoch, S., Fumerola, S., Stephen-Haynes, J.,Edwards-Jones, V., Leaper, D., Strohal, R., White, R., Wicks, G., Young, T. (2010). PHMB and its potential contribution to wound management. Wounds International, Vol 6, No 2.

Background
Chronic wounds are unable to support re-epithelialization, failing to progress through an orderly and timely sequence of repair. These full thickness wounds often present secondarily to diabetes, surgical procedures, inadequate lower extremity vascularization, venous insuciency, or trauma. The use of silver ions has been
demonstrated to be effective against a broad range of bacteria to aid in healing complex wounds and burns. The purpose of this case series is to illustrate the use of silver gelling fiber dressing* containing extra silver ions in full thickness wounds allowing for development of granulation tissue and neoepithelialization of the wound to closure.
Treatment
Four patients with full thickness wounds were treated with silver gelling dressings* impregnated with broad spectrum anti-microbial silver ions. The gelling fiber dressing was placed onto the wound bed where devitalized tissue was removed using sharp and/or ultrasonic debridement. A secondary dressing was applied to secure the primary silver dressing, facilitating a moist healing environment. Adequate offoading and compression therapy was utilized as indicated. The silver gelling fiber was changed every 2-3 days.
Claim Your Free Sample Today
Discover how market-tested quality makes a difference. Request your free sample now and experience the superior performance of our wound dressings firsthand.




Visit Us
North Shangxia Rd. Dongjiang Hi-tech Industry Park, Huizhou, China
As a leader in advanced wound care, Foryou Medical specializes in innovative dressings, hemostatic products, and absorbable biomaterials. Since 2005, we’ve been dedicated to delivering high-quality solutions to meet global healthcare needs.
Showcasing Our Strengths






About Us
Copyright 2023, Hook BZOTech
