

- Who We Are
- DIMES
- Our Products
- Amorphous hydrogel Dressing
- Sliver Wound Gel
- PHMB Antibacterial Alginate Dressing
- Silver Alginate Dressing
- Extra Silver Alginate Dressing
- Extra Silver Gelling Fiber Dressing
- Silver Gelling Fiber Surgical Dressing
- Silver PU Antibacterial Foam Dressing
- Silicone Ag Foam Dressing
- Alginate Dressing
- Silicone Postoperative Dressing
- Foam Dressing
- Medical Hydrogel Dressing
- Silicone Foam Dressing
- Silicone Foam Dressing Border Yoga
- Super Absorbent Dressing
- Gelling Fiber Dressing
- Collagen Wound Dressing
- Collagen Particles
- Silicone Tape
- Silicone Gel Scar Dressing
- Silicone Wound Contact Dressing
- Tech Services
Silver Sustained Release Antibacterial Technology

OptiSil Silicone Perforation Technology

Absorption and Degradation Metabolism Technology

Anti-adhesion Technology
- Blog
- Contact Us
- Case Study
Extra Silver Gelling Fiber Dressing
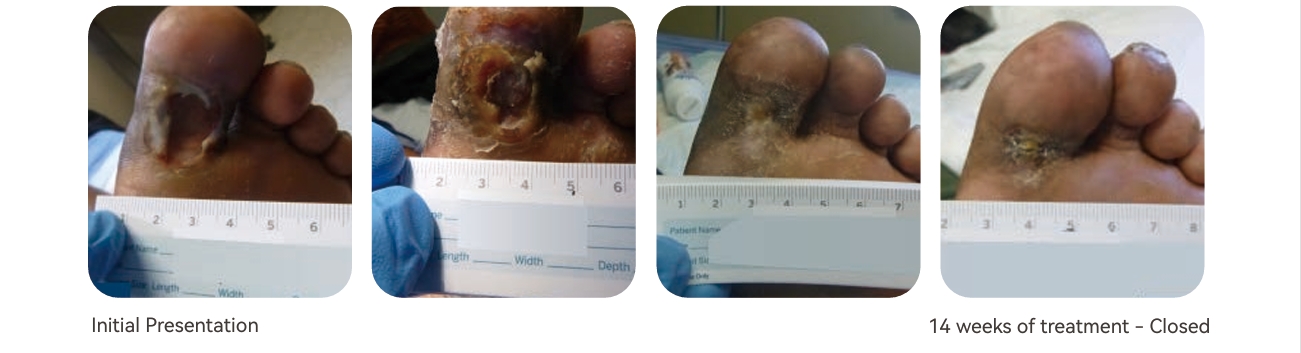
Diabetic Foot Ulcer Left Great Toe (Case 22)
This is a 39 year-old female with history of Diabetes, HTN, HLP, PVD with revascularization, and obesity with recurrent DFUs to the left great toe. The patient was lost to follow up after back surgery returning for evaluation with a DFU, worsening after walking several miles daily for exercise to facilitate weight loss. She reported compliance with bariatric diet, recent weight loss, and glycemic control. She was offoaded with walking boot, as she was unable to tolerate casting due to left lower extremity weakness. MRI revealed osteomyelitis which she received treatment for guided by ID. Dressings were changed 3 times weekly and prn with extra silver gelling fiber dressing.* Duration of treatment – 14 weeks to wound resolution.
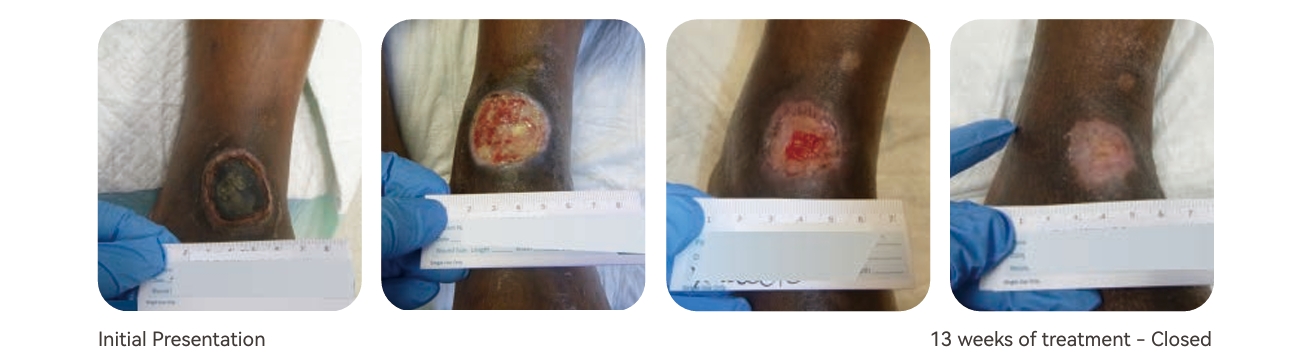
Chronic Ulcer Both Ankle Joints (Case 23)
69 year-old male with history of severe PAD, mixed disease, history of tobacco abuse and CAD presented for eval uation and treatment of chronic ulcers to bilateral ankles. Patient reported his shoes rubbed against his ankles resulting in wounds. Patient initially had limitations with compression due to PAD prior to peripheral bypass grafting as well as successful atherectomy and stenting of the LLE. Wounds resolved in 13 weeks of treatment with aggressive Wound Medicine and extra silver gelling fiber dressings* changed three times weekly.
Diabetic Foot Ulcer Right Foot (Case 24)
Pt is a 59 year-old AAM a PMHx of DM-2, PVD, HTN, HLD, and asthma presented for evaluation of a right plantar DFU. The patient was s/p right foot surgical debridement after developing a callus, which later became infected. Infection was addressed with antibiotic therapy, and the wound offoaded with football wrap and Darco offoading shoe. The patient was educated on glycemic control for optimal wound healing. Dressings were changed three times weekly with extra silver gelling fiber dressing* to reduce bioburden. The wounds resolved after 13 weeks of treatment.
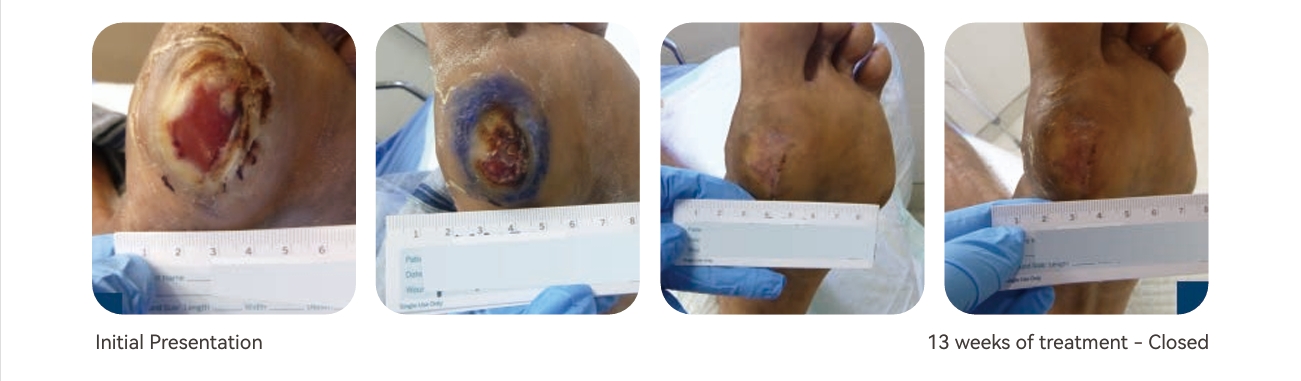
Diabetic Foot Ulcer Left Heel (Case 25)
70-year-old female with DM, CAD, HTN, and ESRD referred for treatment of a left heel DFU. The patient was known to our service after developing a sacral pressure ulcer postoperatively following CABG. The sacral pressure ulcer resolved, although the patient later developed the DFU secondary to pressure following a fall. The wound was debrided weekly, culture obtained, and extra silver gelling fiber dressings* utilized to reduce bioburden and allow granulation and epithelialization. The patient’s heels were offoaded with offoading boots and nutritional support provided to optimize wound healing. The wound resolved in under 13 weeks with dressing changes three times weekly with extra silver gelling fiber dressings.*
Results
Overall wound improvement and closure was appreciated in full thickness wounds. The silver ions assisted in providing an environment where granulation tissue was able to develop allowing for improved epithelialization. The wounds included were an arterial ulcer, a diabetic foot ulcer, and surgical wounds. Patient comorbidities included diabetes and inadequate lower extremity vascularization. Average initial wound size ranged from 3 – 15 cm2. The number of silver gelling fiber applications ranged from 1-13 and time to complete wound epithelialization ranged from 45 – 90 days.
Conclusion
This case series exhibits successful treatment of complex chronic wounds using adequate wound bed preparation and a gelling fiber containing anti-microbial silver ions*. Similar outcomes have been achieved with alginate dressings impregnated with silver ions. Further study is required to determine if Extra Silver Gelling Fiber Dressings improve healing effcacy over other alginate dressings impregnated with silver ions.
References
1. Dissemond J, Böttrich JG, Braunwarth H, et al. Evidence for silver in wound care – meta-analysis of clinical studies from 2000-2015. J Dtsch Dermatol Ges. 2017;15:524–535. [PubMed] [Google Scholar]
2. Silver S. Bacterial silver resistance: molecular biology and uses and misuses of silver compounds. FEMS Microbiol Rev. 2003;27:341–353. [PubMed] [Google Scholar]
3. Warriner R, Burrell R. Infection and the chronic wound: a focus on silver. Adv Skin Wound Care. 2005;18(suppl 1):2–12. [PubMed] [Google Scholar]
Abstract
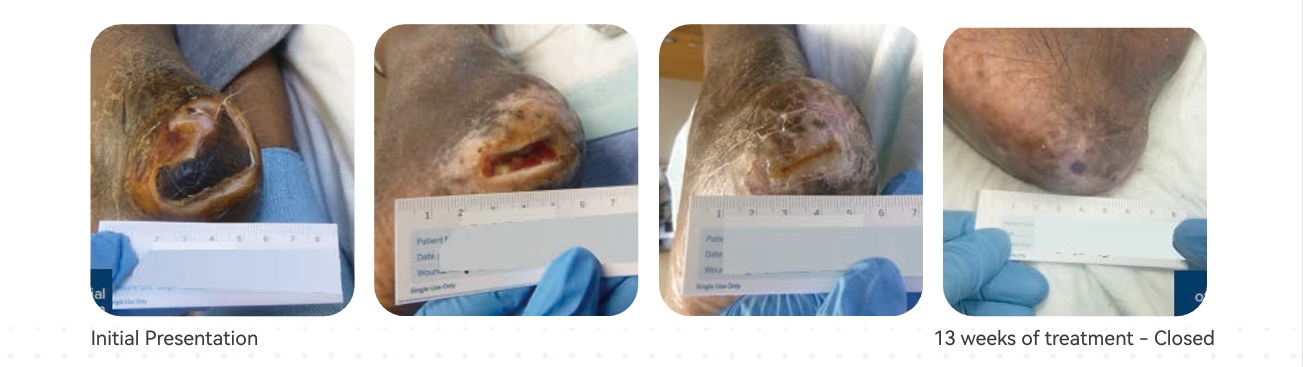
Type I Collagen is the most abundant extracellular matrix protein in the human body and it is clinically effective in the management of Acute & Chronic wounds. Collagen is produced by fibroblasts and it is intricately involved in the (3) phases of wound healing. Collagen primary function is to provide mechanical support and assist in regulating variety of processes, including cell migration, differentiation and proliferation. Use of Collagen dressing has shown to accelerate wound healing, granulation tissue formation, and supports neovascularization, and reduces bacterial infection in the chronic wounds.
Introduction
Collagen is a natural structural protein found in the skin, tendons and bones. Collagen-based biomaterials stimulate and recruit specific cells, such as macrophages and fibroblasts, along the healing cascade in order to enhance and influence wound healing. In acute and chronic wounds delay in proliferation phase causes wound healing to be stalled due to the presence of excessive inflammation and bio-burden. The elevated ratio of MMPs to tissue inhibitors of MMPs leads to excessive extracellular matrix degradation. Use of Collagen dressing during the proliferation phase has shown to accelerate wound healing by reducing elastase levels in a wound environment, disrupting the cycle of chronicity and promoting granulation tissue formation, and supporting neovascularization. There are 28 different types of collagens have been identified in the human body, but the dominant collagen is collagen type I.
Method
This prospective randomized controlled study was conducted at Pro Healthcare Clinic, Dallas, Texas U.S.A. from January to April, 2023. Patients’ inclusion criteria:
Type of wound: Chronic, Present for > 6 weeks
Extent of Tissue Damage: Full thickness Wound, tissue injury extended to the muscle
Patient Age: Between 55 to 90 years
Pre-Albumin Levels: 10 to 40 milligrams per deciliter (mg/dl)
Hgb A1c: 5.7% to 8.0%
All wounds were initially debrided utilizing 7mm dermal curette; swab cultures were collected using Levine’s method and sent to lab for culture and sensitivity testing. Based on culture and sensitivity results; oral antibiotics were ordered for the duration of 10 days. Each wound was evaluated and size was measured on a weekly basis. Luofucon Type-I Bovine Collagen dressing was applied to each wound after being moistened with sterile water, once every 72 hours. Wound square surface area and depth was measured and compared on a weekly basis for 8 weeks.
Calculation Method
The surface area and the depth of each wound was measured each week and subtracted from the surface area and depth measurements of previous week to find the reduction in size and the depth of the wound. These measurements were taken for 8 weeks. The average was calculated after dividing the total reduction in wound area by 7 because initial reduction occurred after the completion of week 1.
Claim Your Free Sample Today
Discover how market-tested quality makes a difference. Request your free sample now and experience the superior performance of our wound dressings firsthand.




Visit Us
North Shangxia Rd. Dongjiang Hi-tech Industry Park, Huizhou, China
As a leader in advanced wound care, Foryou Medical specializes in innovative dressings, hemostatic products, and absorbable biomaterials. Since 2005, we’ve been dedicated to delivering high-quality solutions to meet global healthcare needs.
Showcasing Our Strengths






About Us
Copyright 2023, Hook BZOTech
