

- Who We Are
- DIMES
- Our Products
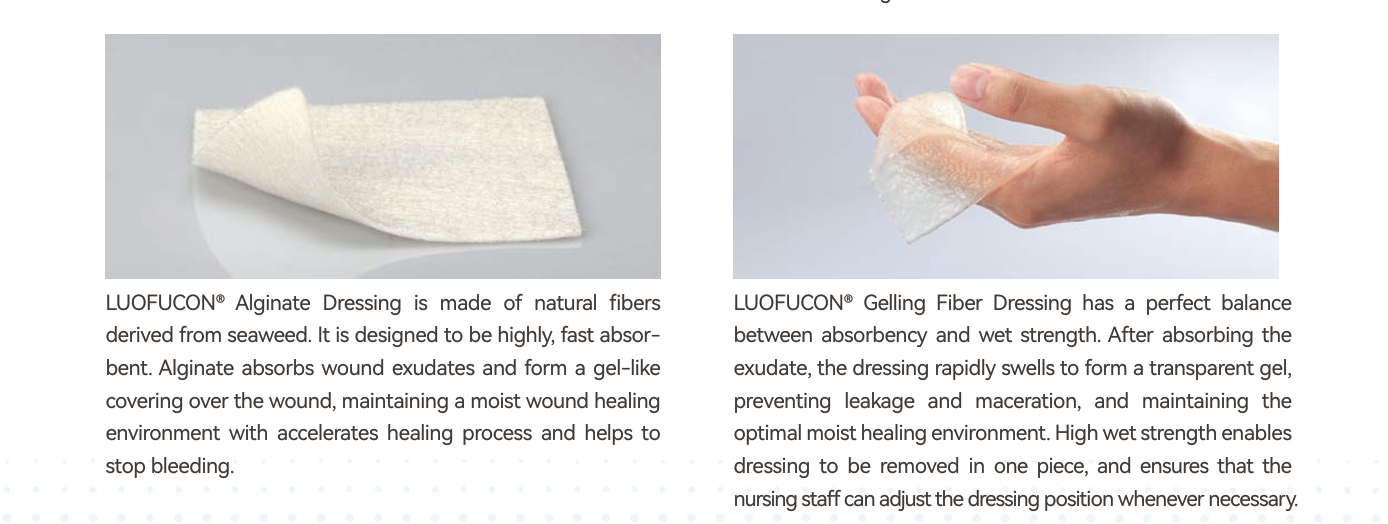
- Amorphous hydrogel Dressing
- Sliver Wound Gel
- PHMB Antibacterial Alginate Dressing
- Silver Alginate Dressing
- Extra Silver Alginate Dressing
- Extra Silver Gelling Fiber Dressing
- Silver Gelling Fiber Surgical Dressing
- Silver PU Antibacterial Foam Dressing
- Silicone Ag Foam Dressing
- Alginate Dressing
- Silicone Postoperative Dressing
- Foam Dressing
- Medical Hydrogel Dressing
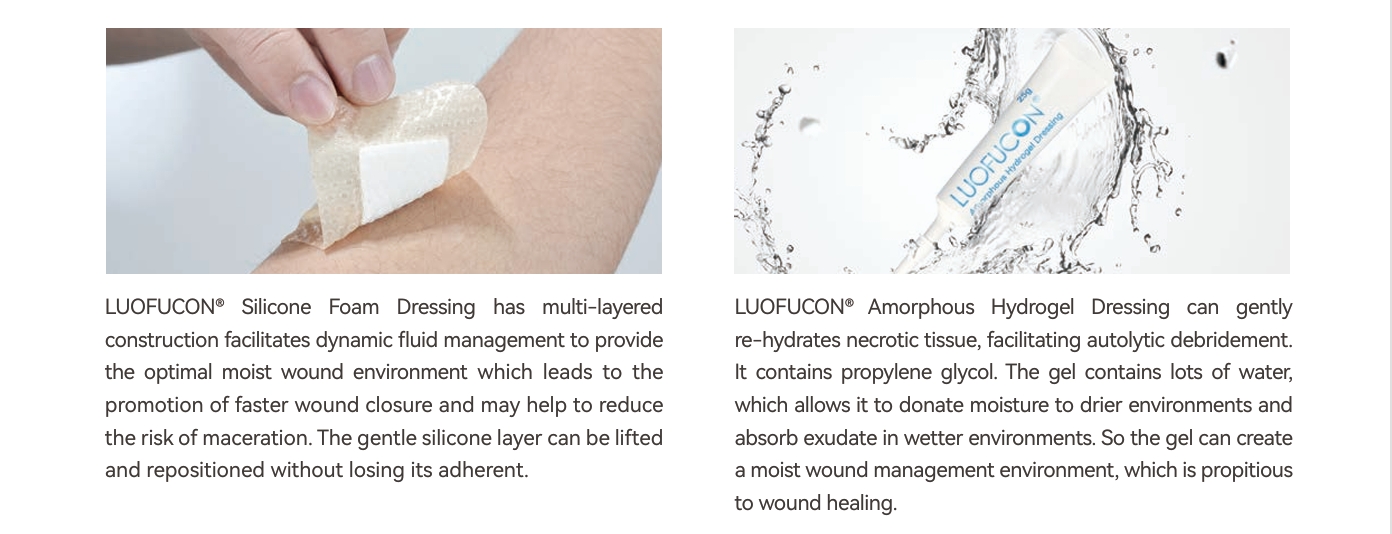
- Silicone Foam Dressing
- Silicone Foam Dressing Border Yoga
- Super Absorbent Dressing
- Gelling Fiber Dressing
- Collagen Wound Dressing
- Collagen Particles
- Silicone Tape
- Silicone Gel Scar Dressing
- Silicone Wound Contact Dressing
- Tech Services
Silver Sustained Release Antibacterial Technology

OptiSil Silicone Perforation Technology

Absorption and Degradation Metabolism Technology

Anti-adhesion Technology
- Blog
- Contact Us
- Case Study
Silicone Foam Dressing
Surgical Wound Upper Arm (Case 1)
21 yrs. old male with a surgical wound of the right upper arm status post amputation due to osteomyelitis. Patient medical history includes smoking and illicit drug abuse. Wound made remarkable progress during the (8) weeks of clinical trial. Wound bed granulated appropriately without any maceration and adhesion.

Surgical Wound Full Thickness-left Hip (Case 2)
82 yrs. old female with a non-healing surgical wound of the left hip associated with a hip replacement surgery completed approximately 14 months ago. Patient’s medical history included diabetes mellitus T-II, hypertension, hyperlipidemia, morbid obesity, and osteomyelitis. Due to rolled wound margins and significant tunneling plastic surgery evaluation was planned. Sharp debridement completed on the wound initially and after 7 weeks of dressing changes, improved granulation was noted and the patient was referred to a Plastic surgeon for the surgical closure. Wound was surgically closed and 100% wound closure was achieved within 8 weeks.
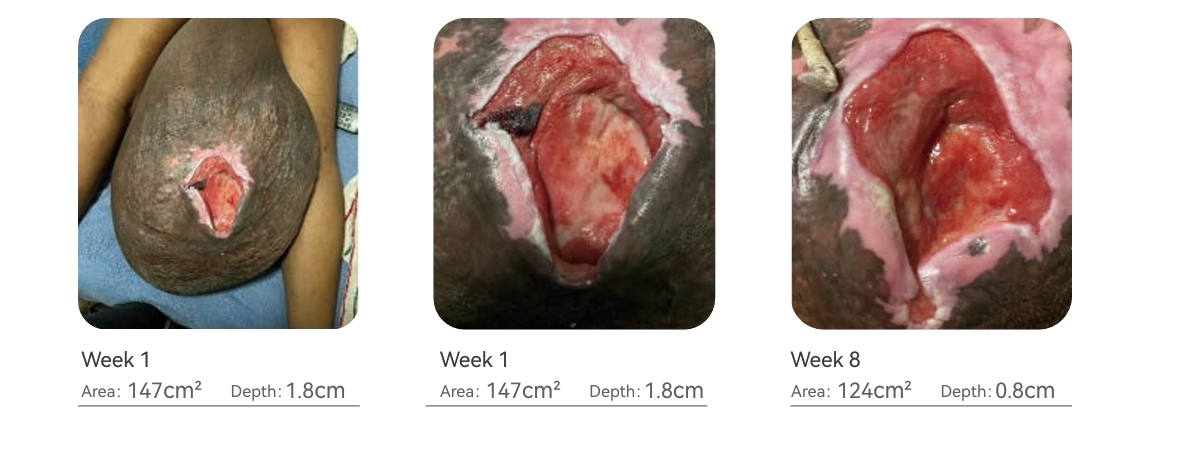
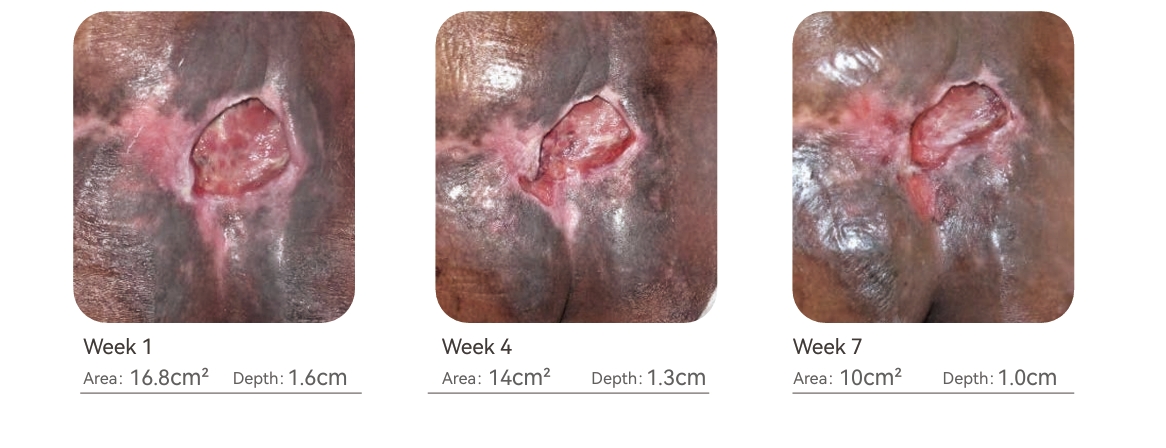
Stage IV Pressure Ulcer Scrotum (Case 3)
54 yrs. old male with a stage IV pressure ulcer of the Scrotum. Patient has enlarged scrotum due to the diagnosis of Hydrocele. Patient’s medical history includes hypertension, diabetes mellitus Type II and hyperlipidemia. Due to difficulty in off-loading of the affected area, complete wound closure was not achieved during the 8 weeks of treatment but increased granulation tissue and wound contraction was noted during the evaluation period. Moderate exudate was also well managed with the dressings.
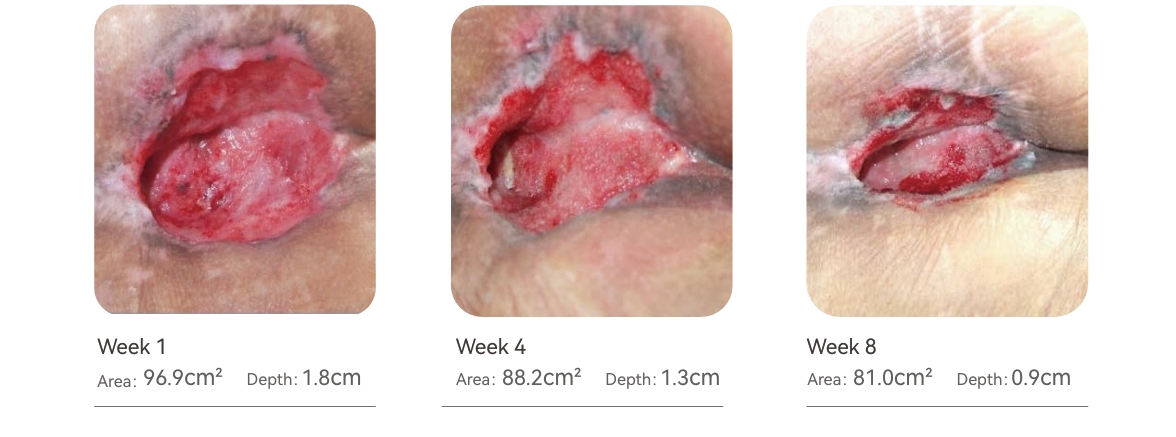
Stage IV Pressure Ulcer Coccyx Region (Case 4)
66 yrs. old male with a stage IV pressure ulcer of the Coccyx region. Pressure injury caused tissue damage extended to the muscle with moderate drainage. Patient confined to bed acquired pressure ulcer due to bowel & bladder incontinence and lack of pressure relief. Patient’s medical history includes hypertension, hyperlipidemia, chronic kidney disease and malnutrition. Due to malnutrition and compliance issues wound closure was not achieved during the 8 weeks of treatment but significant improvement was noted during the evaluation period.distribution allowed the wound to make significant progress during the evaluation period.

Stage IV Pressure Ulcer Sacral Region (Case 5)
70 yrs. old female with a stage IV pressure ulcer of the Sacral region. Patient confined to bed acquired pressure ulcer due to bowel & bladder incontinence, bowel bladder incontinence, and malnutrition. Patient’s medical history includes congestive heart failure, hypertension, diabetes mellitus T-II, hyperlipidemia, chronic kidney disease and malnutrition. Wound had tissue damage extended to the muscle with tunnelingat 12 o clockand had copious serous drainage.Due to malnutrition and complex concurrent medical issues wound closure was not achieved during the 8 weeks of treatment but significant improvement was noted during the evaluation period.
Stage IV Pressure Ulcer Sacrum (Case 6)
68 yrs. old male with a stage IV pressure ulcer of the Sacrum. Patient s/p CVA with the right sided weakness and confined to bed acquired tissue injury due to incontinence and lack of off-loading. Patient’s medical history includes hypertension, diabetes mellitus Type II, hyperlipidemia and malnutrition. Due to malnutrition, elevated HgbA1c (9.5%) wound closure was not achieved during the 8 weeks of treatment but significant improvement was noted during the evaluation period. Full thickness wound with tissue damage was extended to the muscle and dressing changes with off loading and appropriate pressure distribution allowed the wound to make signifi cant progress during the evaluation period.

Stage IV Pressure Ulcer Sacro-coccyx Region (Case 7)
78 yrs. old female with a stage IV pressure ulcer of the sacro-coccyx region due to incontinence, bed confinement, malnutrition and advanced age. Pressure injury caused tissue damage extended to the muscle and bone with copious serous drainage and circumferential undermining. Patient medical history includes congestive heart failure, CVA, hypertension, and end stage renal disease. Wound made good progress during the (8) weeks of clinical trial. Wound bed was actively granulating and contracting but patient was hospitalized due to CHF exacerbation.
Stage IV Pressure Ulcer Left Hip (Case 8)
88 yrs. old female with a stage IV pressure ulcer of the left hip due to incontinence, bed confinement, malnutrition and end stage Alzheimer’s disease. Malnutrition and pressure injury caused tissue breakdown extended to the muscle and bone with copious sanguineous drainage and circumferential undermining. Patient medical history includes dementia, hypertension, and diabetes type II . Wound made significant progress during this evaluation period and showed positive effects of the dressing on the wound bed. Patient was on Hospice services.

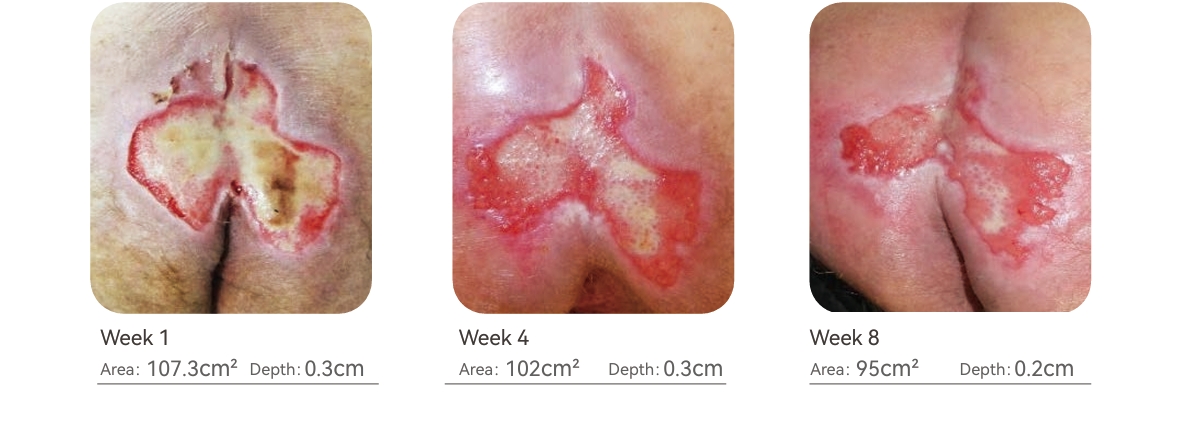
Stage III Pressure Ulcer Bilateral Buttocks (Case 9)
68 yrs. old female with a stage III pressure ulcer of bilateral buttocks. Pressure injury caused tissue damage extended to the subcutaneous tissue with copious serous-sanguineous drainage. Patient confined to bed acquired pressure ulcer due to bowel & bladder incontinence and malnutrition. Patient’s medical history includes smoking, coronary artery disease, hypertension, hyperlipidemia, and depression. Due to malnutrition and compliance issues wound closure was not achieved during the 8 weeks of treatment but significant improvement was noted. Dressing changes improved the wound bed and promoted active granulation.
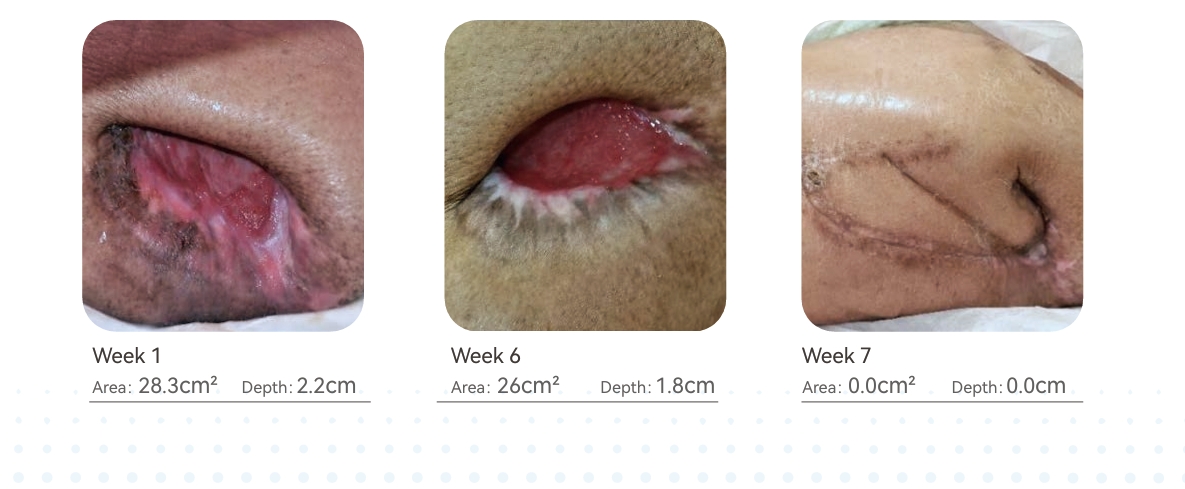
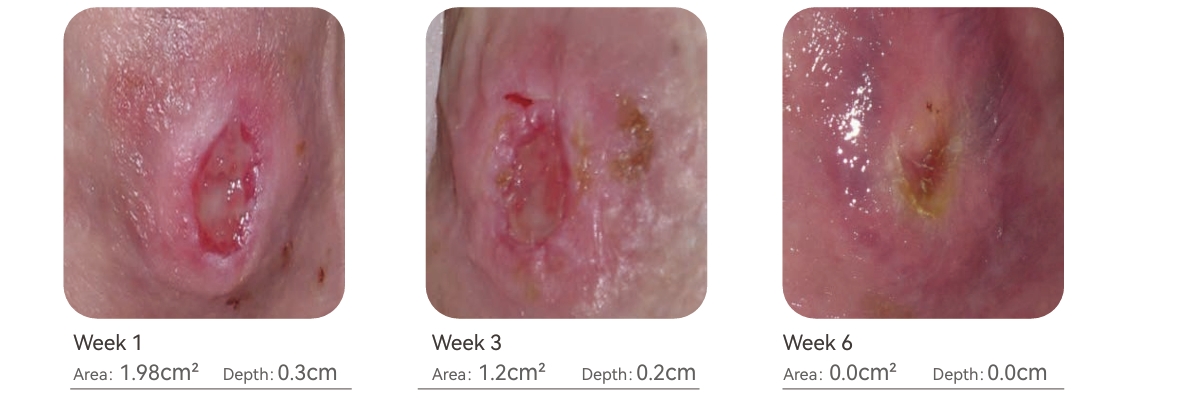
Stage III Pressure Ulcer Ankle (Case 10)
46 yrs. old female with a stage III pressure ulcer of the left ankle lateral aspect. Patient medical history includes; Multiple Sclerosis, bed confinement, generalized weakness, and hypothyroidism. During the (6) weeks treatment 100% wound closure was achieved. Off loading and dressing changes were effective in the timely closure of the wound.
Results
All (10) patients were evaluated weekly and wound surface area (cm2) & depth were carefully measured and recorded. In all (10) patients, wound contraction, tissue regeneration and bio-burden management were significant and no critical colonization was recorded. During the evaluation period all wounds showed improvement in size, drainage, and the percentage of granulation tissue present in the wound.
Discussion
This clinical case study was focused on maintaining a therapeutic environment during the proliferation phase of wound healing in full thickness wounds. In each clinical case, bio-burden of the wound was appropriately addressed initially through the culture & sensitivity testing and oral antibiotics. Application of Calcium Alginate with Silver (Ag) as a primary dressing in all clinical cases, was effective in maintaining wound bio-burden level and maintaining a moist wound environment ideal for regeneration of connective tissue. Critical colonization in wounds causes extended inflammation and thus delays the wound healing. Silicone foam was utilized as a secondary dressing in all clinical cases and found to be extremely effective due to its properties such as, protecting the wound base from external trauma, protecting the wound from external contamination, maintaining optimal vapor transfer rate and gaseous exchange necessary for cell metabolism, capability of absorbing exudate from the wound and preventing peri-wound skin maceration and conforming to the wound shape and size.
Conclusion
Based on our clinical evaluation results, it is concluded that Silicone foam dressing with adhesive borders and Calcium Alginate with Silver (LUOFUCON® ) were clinically effective in the management of full thickness wounds in any healthcare setting.
References
1. Mervis JS, Phillips TJ. Pressure ulcers: Pathophysiology, epidemiology, risk factors, and presentation. J Am Acad Dermatol. 2019;81(4):881–890.
2. Horn SD, Bender SA, Ferguson ML. The National Pressure Ulcer Long-term Care Study: pressure ulcer development in long-term care residents. J Am Geriatr
Soc. 2004;52:359–367.
Stage IV Pressure Ulcer Left Ankle (Case 11)
Background
Ms. A.W. is an 80-year-old female who is bed bound and lives with her niece in their private home located in Dallas, Texas, USA. Patient has Dementia, Protein Calorie Malnutrition, Dysphagia with a Gastrostomy tube, Arterial insufficiency to the bilateral lower extremities with ABI of 0.4, Contractures to both knees, and Generalized Weakness. Due to immobility and her bed confinement status; Ms. A.W. developed a stage IV pressure ulcer on her left ankle.
Abstract
Initial assessment of the wound reveals tissue injury extending to the bone with Peri-Wound skin maceration due to moderate serious drainage. Wound was tender to the touch with a pain level rated 6 on a scale of 1-10. There was a mild odor to the wound
Physiological Factors
•Contractures of the bilateral knees
• Immobility & confined to bed
• Generalized weakness
Clinical Factors
• Dementia
• PAD Arterial Insufficiency – ABI: 0.4 (Range: 0.9-1.3)
• Malnutrition related to Dysphagia | Pre-Albumin: 12 (15-36)
• Advanced age not a candidate for re-vascularization
• Pain due to Ischemia and pressure ulcer
• Dementia
• PAD Arterial Insufficiency – ABI: 0.4 (Range: 0.9-1.3)
• Malnutrition related to Dysphagia | Pre-Albumin: 12 (15-36)
• Advanced age not a candidate for re-vascularization
• Pain due to Ischemia and pressure ulcer
Treatment
① Highly absorbent to manage the moderate serous drainage and to prevent peri-wound skin maceration.
② Offers padding to the wound site and prevents further trauma to the wound base.
③ Easy application and removal. Silicone borders appropriate for thin elderly skin; that is high risk for breakdown.
④ Use of 4 x 4 Silicone Foam dressing with adhesive borders allowed The family to change the dressings without any complications such as too tight wrappings that may have caused further circulation issues.

Conclusion
Luofucon Silicone Foam Dressing was found to be effective in managing the Stage IV Pressure Ulcer of Ms. A.W.

Stage III Pressure Ulcer ( Back )
Stage IV Pressure Ulcer ( Sacrum )(Case 12)
Background
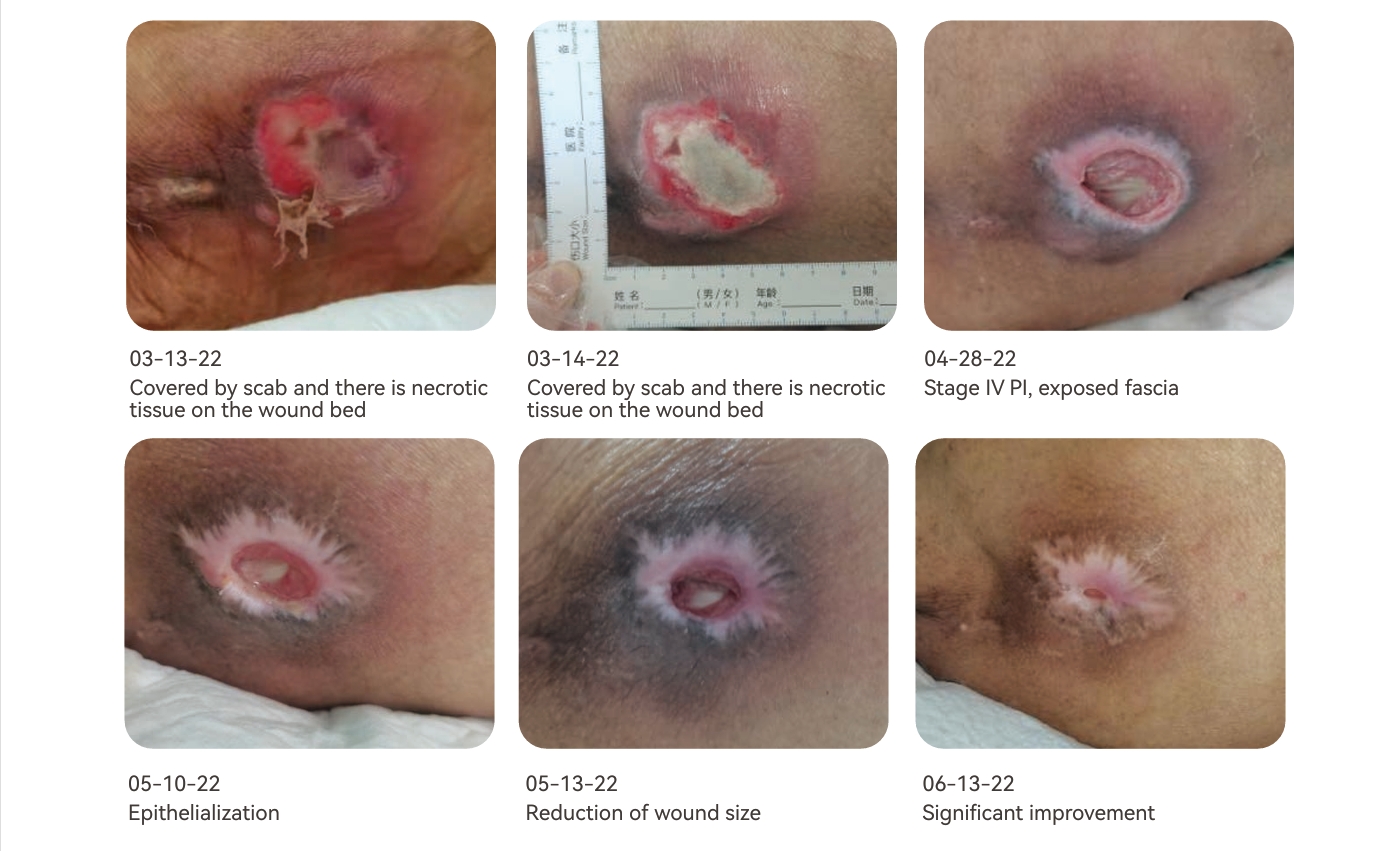
Mrs. WLM is 93 years old, has been in bed for a long time, unwilling to turn over and is so thin. Wound introduction: Stage 3 PI of back and stage IV PI of sacrum.
Abstract
Intervention of treatment was performed during 2022.3.13 to 2022.6.13 Conventional nursing with advanced wound care dressing were performed. The whole process was 13 weeks, while the first 4 weeks for intensive intervention, and the last 9 weeks for general nursing. LUOFUCON® Gelling Fiber Dressing, Silicone Foam Dressing,Silicon Tape were used for this patient during the care routine.

Treatment
① Disinfect the wound with iodophor, clean it with normal saline, and slightly dry it with gauze. If feasible, perform sharp debridement on the wound first and then repeat above disinfection routine and dry the wound. Moisturize LUOFUCON® Gelling Fiber Dressing with normal saline, cover it on the wound bed, and use LUOFUCON® Silicone Foam Dressing Border as secondary dressing to protect the wound. This period starts from March 13, 2022 and lasts until April 28, 2022. Autolytic debridement is mainly used, and it is replaced dressing every 48 hours until the wound base presents 100% pink granulation.
② Disinfect the wound with iodophor, clean it with normal saline. LUOFUCON® Gelling Fiber Dressing is cut to the appropriate size to fill the cavity and sinus, leaving no gaps and the tightness is appropriate. At the epithelial stage, there is less wound exudate. At this time, it is necessary to flexibly choose whether to fill the wound with LUOFUCON® Gelling Fiber Dressing according to exudate and applica tion requirements. LUOFUCON® Silicone Foam Dressing is used for secondary dressing, and LUOFUCON® Silicon Tape is used for auxiliary fixation. This period starts from April 28, 2022 and lasts until June 13, 2022. It was mainly based on healing management and was replaced dressing every 48 hours until the back wound was completely healed and the sacral wound was significantly improved.
Figure of the healing process of the back wound
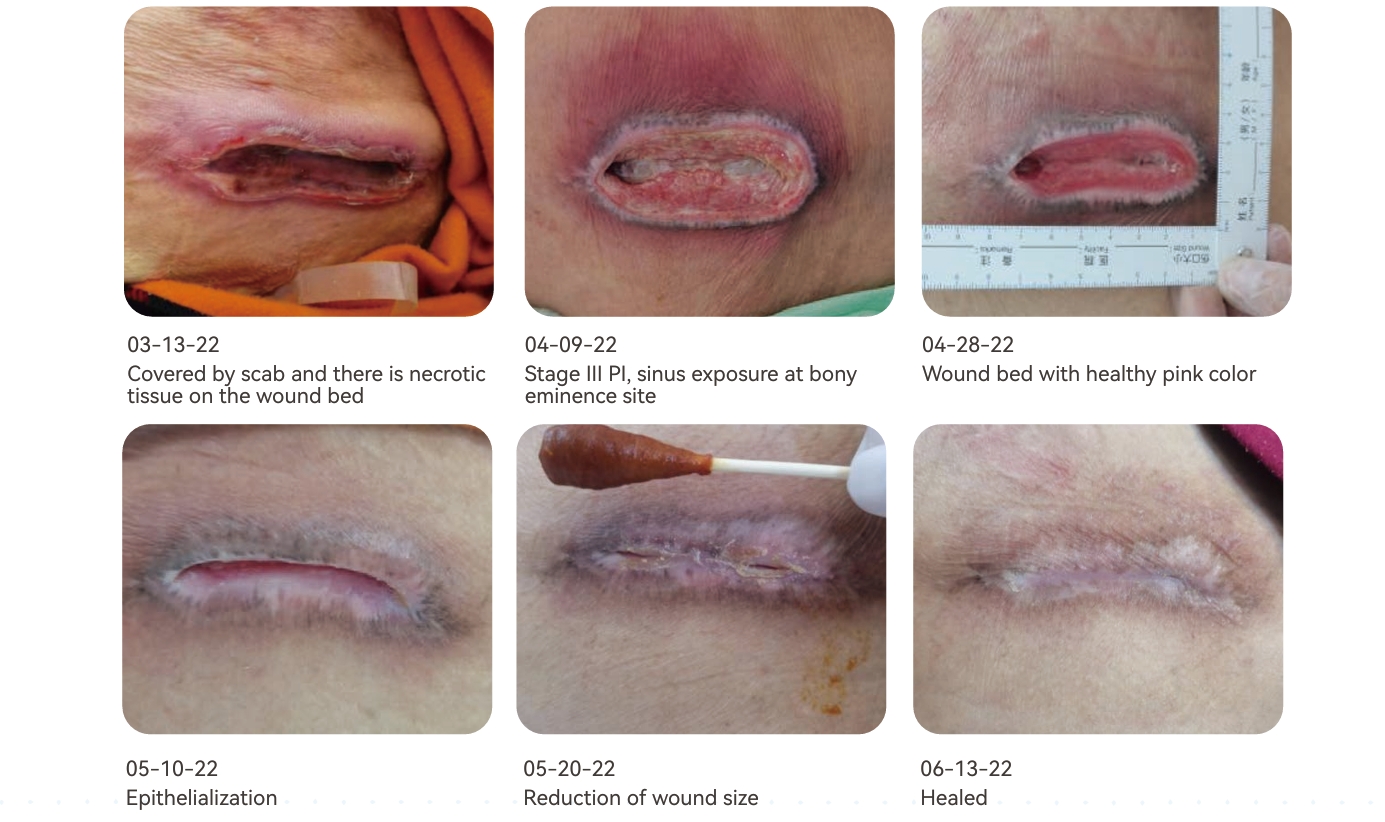
Figure of the healing process of the sacral wound
Conclusion
The 93-year-old suffered from two PI in the back and sacrum. Due to her old age and intolerance to surgery, according to the evaluation, autolysis debridement combined with sharp debridement was adopted to minimize invasive operations. Use the following dressings according to the amount of wound exudate and nursing conditions to achieve a better moisture balance.
LUOFUCON® Gelling Fiber Dressing can be used as absorbent dressings to manage the excessively wet exudate environment of the wound, and can also be used as moisturizing materials/water supply materials to adjust the excessively dry wound surface environment. With the combination of LUOFUCON® Gelling Fiber Dressing and normal saline, the dressing can quickly form a semitransparent gel, soften and liquefy the scab and slough, and finally remove the scab to achieve the goal of autolysis debridement.
LUOFUCON® Silicone Foam Dressing Border dynamically manages the exudate, provides a moist healing environment for the wound, and protects the wound and surrounding skin from additional trauma. It plays an important role in providing a suitable environment for the wound healing.
LUOFUCON® Silicone Foam Dressing is a new sterile advanced wound care dressing, which absorbs a large amount of exudate. It is soft and comfortable, can protect the wound at the bony eminence sites and provide good cushioning effect.
LUOFUCON® Silicon Tape is used for auxiliary fixation, providing gentle care for the wound together with LUOFUCON® Silicone Foam Dressing. The silicone layer has a mild viscosity, and there will be no residual glue left at the sticking place when it is removed.
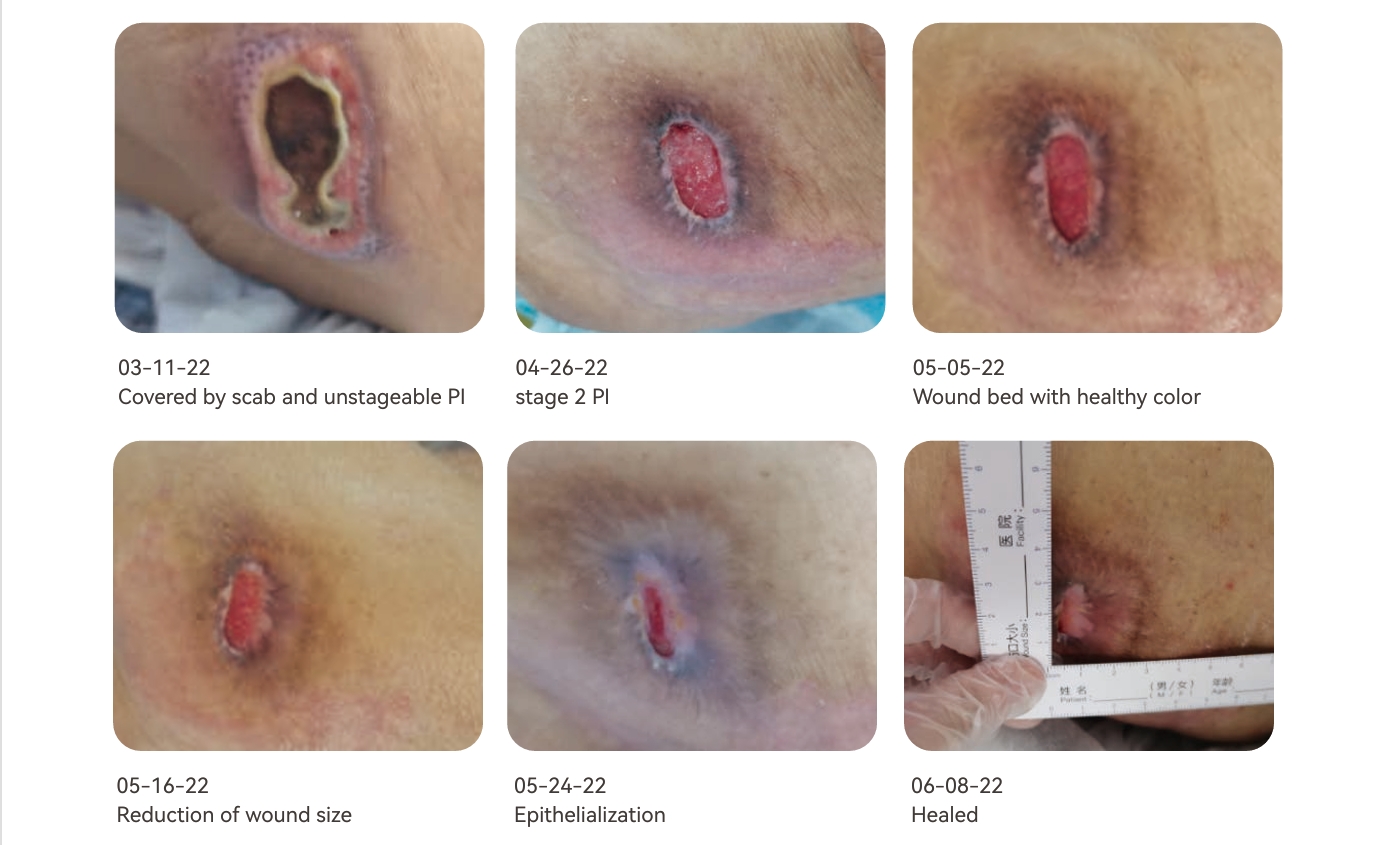
Stage II Pressure Ulcer Left Hip (Case 13)
Background
The 78 years old disabled elderly, who is unwilling to turn over due to long-term lying in bed, is thin, and has a total of 3 pressure injuries (sacrococcygeal wound, right hip wound, and left hip wound). Due to asthma, oxygen inhalation is required, and prone position cannot be taken. And because the sacrococcygeal wound and right hip wound were seriously, the left hip was still under long-term pressure, which increased the difficulty of nursing. This case only shows the nursing process of the left hip wound.
Abstract
Intervention of treatment was performed during 2022.3.13 to 2022.6.13 Conventional nursing with advanced wound care dressing were performed. The whole process was 13 weeks, of which, from March 13 to April 26 is the time for intensive intervention, and the follow-up will be transferred to general care. LUOFUCON® Gelling Fiber Dressing, LUOFUCON® Silicone Foam Dressing , LUOFUCON® Alginate Dressing were used for this patient during the care routine.

Treatment
① Disinfect the wound with iodophor, clean it with normal saline, and slightly dry it with gauze. If feasible, perform sharp debridement on the wound first and then repeat above disinfection routine. Moisturize LUOFUCON® Gelling Fiber Dressing with normal saline, cover it on the wound bed, and use LUOFUCON® Silicone Foam Dressing Border as secondary dressing to protect the wound. This period starts from March 11, 2022 and lasts until April 26, 2022. It is replaced dressing every 48 hours, the patient’s wound changes from unstageable PI to stage 2 PI, autolysis debridement effect is significant, and the base of wound bed presents 100% pink granulation.
②Disinfect the wound with iodophor, clean it with normal saline. Cover the wound bed with LUOFUCON® Alginate Dressing, and then use LUOFUCON® Silicone Foam Dressing Border as secondary dressing. On May 5, 2022 the wound began to shrink and gradually epithelialized, and the wound healed on June 8 2022.
Conclusion
The 78 years old disabled elderly suffered from three PI in the hip and sacrum. According to the evaluation, autolysis debridement combined with sharp debridement was adopted to minimize invasive operations. Use the following dressings according to the amount of wound exudate and nursing conditions to achieve a better moisture balance.
LUOFUCON® Gelling Fiber Dressing can be used as absorbent dressings to manage the excessively wet exudate environment of the wound, and can also be used as moisturizing materials/water supply materials to adjust the excessively dry wound surface environment. With the combination of LUOFUCON® Gelling Fiber Dressing and normal saline, the dressing can quickly form a semitransparent gel, soften and liquefy the scab and slough, and finally remove the scab to achieve the goal of autolysis debridement. LUOFUCON® Gelling Fiber Dressing can bring convenience to nursing staff and shorten the dressing change time required for acute debridement.
LUOFUCON® Silicone Foam Dressing Border dynamically manages the exudate, provides a moist healing environment for the wound, and protects the wound and surrounding skin from additional trauma. It plays an important role in providing a suitable environment for the wound healing.
LUOFUCON® Alginate Dressing is natural, soft, and has high absorption capacity. It forms a moist gel protective layer between the wound and the dressing, creating a moist healing environment, and also have a good conductivity and good compliance.
REFERENCES
1. European Pressure Ulcer Advisory Panel,National Pressure Injury Advisory Panel,Pan Pacific Pressure Injury Alliance.Prevention and treatment of pressure ulcers /injuries: clini cal practice guideline[S].EPUAP /NPIAP /PPPIA: 2019.
2. Reaper S,Green C,Gupta S,et al.Inter-rater reliability of the Reaper Oral Mucosa Pressure Injury Scale ( ROMPIS) :a novel scale for the assessment of the severity of pressure injuries to the mouth and oral mucosa[J]. Aust Crit Care,2017,30( 3) : 167-171.
3. Baumgarten M,Margolis D,van Doorn C,et al. Black/White differences in pressure ulcer incidence in nursing home residents[J]. J Am Geriatr Soc,2004,52( 8) : 1293-1298.
4. Verbrugghe M,Beeckman D,van Hecke A,et al.Malnutri tion and associated factors in nursing home residents: across-sectional,multi-centre study[J]. Clin Nutr,2013,32( 3) : 438-443.
5. Wojcik A,Atkins M,Mager D R.Dietary intake in clients with chronic wounds[J].Can J Diet Pract Res,2011,72( 2) :77-82.
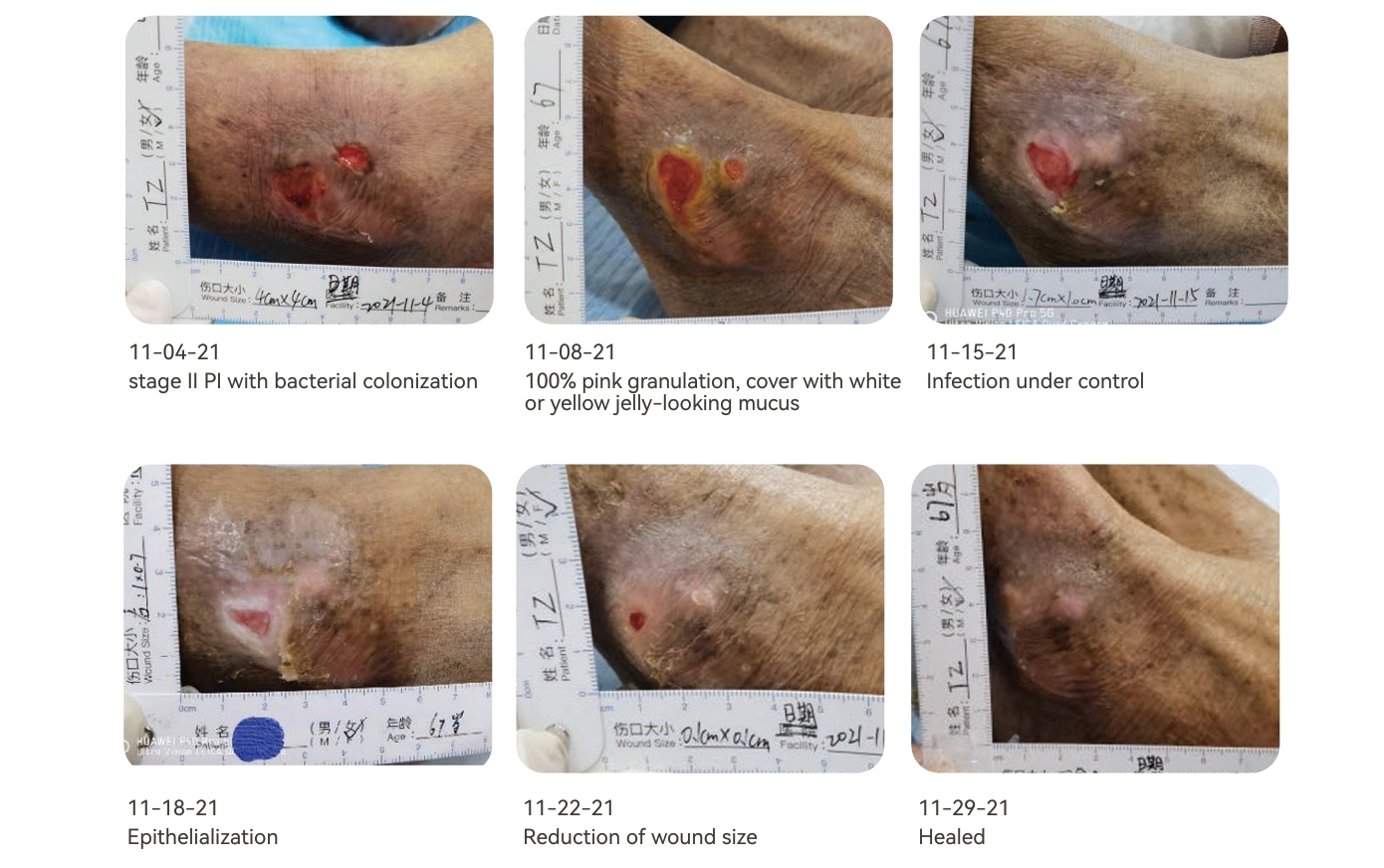
Stage II Pressure Ulcer Right Ankle (Case 15)
Background
Ms. Tang, 67 years old, has been suffering from diabetes for more than 10 years. She takes melbine daily to control blood sugar, and has been in bed for a long time. Two weeks ago, she came to the wound stoma department in a wheelchair for treatment of pressure ulcer on her right ankle.
Abstract
Intervention of treatment was performed during 2021.11.4 to 2021.11.29, the whole process was 4 weeks, in which the anti-infection management was mainly carried out in the early stage, and then it was converted to general care. LUOFUCON® Silicone Foam Dressing , Hydrocolloid Dressing were used for this patient during the care routine.
Treatment
① Disinfect the wound with iodophor, clean it with normal saline, and slightly dry it with gauze. Amino Acid Compound Ointment was used to moisturize the wound, and then covered LUOFUCON® Silicone Foam Dressing Border as secondary dressing to protect the wound, and the dressing was changed twice a week. At the same time, instruct patients and their families to change their positions regularly, master the skills of changing their positions correctly, and avoid dragging and other actions, so as to reduce local pressure and friction. Keeps skin clean and dry. Choose foods rich in high-quality protein and vitamins, and eat a light diet.
② The Amino Acid Compound Ointment used due to the dry wound causes the wound to be macerated, and it does not have antibacterial effect, resulting in the formation of biofilm in the wound. Remove biofilm through Conservative Sharp Wound Debridement, and then apply iodophor gauze to control infection. LUOFUCON® Silicone Foam Dressing Border is not suitable for use with iodophor gauze, so the secondary dressing will be replaced with ordinary dry gauze during this period to increase the permeability of the wound. Change dressing once a day and observe the wound healing.
② After the wound infection is controlled, the topical antibacterial agent is no longer used, and the Hydrocolloid Dressing is used to promote the epithelization of the wound. The use of LUOFUCON® Silicone Foam Dressing Border as a secondary dressing can effectively manage the exudate, buffer the pressure, protect the wound, and maintain a moist wound healing environment.
② The obvious wound healing indicates that the nursing management is effective and should be maintained. The frequency of dressing change reduced to once a week until the wound is healed.
Conclusion
There is no obvious necrotic tissue in the wound, and the biofilm cannot be seen by eyes in the early stage of reces sive infection unless when it reaches a certain degree will it form gelatinous membrane-like substances on the wound. For chronic wounds, the risk of wound infection should be fully assessed.
For wounds with high risk of infection or latent infection, bacterial culture should be carried out early to guide treatment; use wet dressing carefully to avoid obvious infection; appropriate use of topical broad-spectrum antibacterial agents, such as silver dressings, iodoform gauze, etc., can also use a wet iodophor gauze,dilute iodophor to soak or other methods to reduce the Bioburden of the wound.
LUOFUCON® Silicone Foam Dressing Border can effectively manage the exudation, maintain a moderate moist environment, especially suitable for wounds with better infection control, or in the granulation stage and epithelial stage. Foam dressing combined with hydrocolloid dressing can effectively promote epithelization.
REFERENCES
1. Chen Lijuan, Sun Linli, Liu Lihong, et al. An interpretation of the International Clinical Practice Guideline for the prevention and treatment of pressure ulcers/injuries 2019.2020,35 (13):41-43,51. DOI:10.3870/j.issn.1001-4152.2020.13.041.
2. Hu Ailing, Yu Ting, Wen Jiahui. Interpretation of expert standard for nursing care of patient with chronic wound.2018,18(1):15-18. DOI:10.3969/j.issn.1672-1756.2
3. Trengove N J , Stacey M C , Macauley S , et al. Analysis of the acute and chronic wound environments: the role of proteases and their inhibitors[J]. Wound Repair & Regeneration, 2010, 7(6):442-452.
4. Siddiqui A R , Bernstein J M . Chronic wound infection: Facts and controversies[J]. Clinics in Dermatology, 2010, 28(5):519-526.
5. Imanaka K , Kyo S , Asano H , et al. [Coronary artery bypass grafting in patients undergoing chronic hemodialysis: importance of wound healing and hypoproteinemia].[J]. Journal of Cardiology, 2005, 45(2):47.
6. Sores P . Pressure, hygiene, spasticity and chronic infection are the important local factors in pressure ulceration. Hypoproteinemia, nutritional deficiency and anemia are the systemic factors. Careful attention to local wound care and dietary supplements is[J]. Skin, 1983.
Surgical Wound Dehiscence Left Lower Limb (Case 17)
Background
Ms. Tang, 62 years old, took the great saphenous vein of the left lower limb for bypass surgery due to acute myocardial infarction emergency one month ago, and now came to the clinic on November 4, 2021 because of the nonunion of the wound after the leg surgery. She has suffered from diabetes and hypertension for many years, but has routine control with medication.
Abstract
Intervention of treatment was performed during 2021.11.4 to 2021.11.22, the whole process was 3 weeks, in which the anti-infection management was mainly carried out in the early stage, and then it was converted to general care. LUOFUCON® Silicone Foam Dressing , Hydrogel Dressing and Silver Dressing were used for this patient during the care routine.
Treatment
① Disinfect the wound with iodophor, clean it with normal saline, and slightly dry it with gauze. Choose Silver Dressing as primary dressing to control infection, and then covered LUOFUCON® Silicone Foam Dressing Border as secondary dressing to protect the wound, and the dressing was changed twice a week.
②After the wound infection is controlled, the Silver Dressing is no longer used, and the Hydrogel Dressing is used to maintain moist environment and promote epithelization. The use of LUOFUCON® Silicone Foam Dressing Border as a secondary dressing can effectively manage the exudate, buffer the pressure, protect the wound.
③ The wound healed completely. Educate the patient to keep her skin clean, use skin protectors to care for newborn skin.

Conclusion
LUOFUCON® Silicone Foam Dressing Border can effectively manage the exudation, maintain a moderate moist environment, especially suitable for wounds with better infection control, or in the granulation stage and epithelial stage. The Hydrogel Dressing can create an environment suitable for wound healing by adjusting the humidity of the wound surface. Foam dressing combined with Hydrogel Dressing can effectively promote epithelization.
REFERENCES
1. World Union of Wound Healing Societies (WUWHS) Consensus Document. Surgical wound dehiscence: improving prevention and outcomes. Wounds International, 2018.
2. Hu Ailing, Yu Ting, Wen Jiahui. Interpretation of expert standard for nursing care of patient with chronic wound.2018,18(1):15-18. DOI:10.3969/j.issn.1672-1756.2.
3 . Liu W Y , Liu Y , Zhang N N , et al. Clinical analysis of orthopaedic sterile surgical incision infection and nursing countermeasures[J]. Chinese Journal of Nosocomiology, 2011, 21(13):2689-2690.
4. Jiang X Y . Related factors for surgical incision infections in department of orthopedics and nursing countermeasures[J]. Chinese Journal of Nosocomiology, 2012. Hahler B . Surgical wound dehiscence.[J]. Medsurg nursing : official journal of the Academy of Medical-Surgical Nurses, 2006, 15(5):296.
5. Hahler B . Surgical wound dehiscence.[J]. Medsurg nursing : official journal of the Academy of Medical-Surgical Nurses, 2006, 15(5):296.
6. Sergio B , Mario A , Gaetano M . INFECTION AND DEHISCENCE OF AN ABDOMINAL SURGICAL WOUND AFTER REVERSION ‒ THE CORRECT USE OF ADVANCED WOUND DRESSINGS[C]//EWMA 2012. 2012.

Background
Difficult-to-heal, full-thickness wounds often present in the setting of diabetes, surgical procedures, vascular disease, or trauma. Chronic wounds are often unable to support re-epithelialization and can require dermal substitutes or skin grafts to heal. Chronic wounds are complicated by bacterial colonization, development of biofilm, and often infection2. Topical antiseptic/antimicrobial preparations such as polyhexamethylene biguanide (PHMB) can significantly decrease bioburden1 and speed healing time2. The use of alginate dressings has been reported to successfully heal complex wounds and burns. The purpose of this case series is to describe the use of alginate dressings containing PHMB (Alg/PHMB) in full thickness wounds to prevent infection, generate vascularized tissue, and encourage neoepithelialization.
Treatment
Four patients with full thickness wounds were treated with alginate dressings impregnated with PHMB*. Alg/PHMB was placed onto wounds that had been prepared with sharp and/or ultrasonic debridement. A cover dressing was applied to secure the Alg/PHMB to maintain appropriate moisture balance. The wounds were offioaded and/or compressed as medically indicated. Alg/PHMB dressings were reapplied every 2 – 3 days.
Claim Your Free Sample Today
Discover how market-tested quality makes a difference. Request your free sample now and experience the superior performance of our wound dressings firsthand.




Visit Us
North Shangxia Rd. Dongjiang Hi-tech Industry Park, Huizhou, China
As a leader in advanced wound care, Foryou Medical specializes in innovative dressings, hemostatic products, and absorbable biomaterials. Since 2005, we’ve been dedicated to delivering high-quality solutions to meet global healthcare needs.
Showcasing Our Strengths






About Us
Copyright 2023, Hook BZOTech
