

- Who We Are
- DIMES
- Our Products
- Amorphous hydrogel Dressing
- Sliver Wound Gel
- PHMB Antibacterial Alginate Dressing
- Silver Alginate Dressing
- Extra Silver Alginate Dressing
- Extra Silver Gelling Fiber Dressing
- Silver Gelling Fiber Surgical Dressing
- Silver PU Antibacterial Foam Dressing
- Silicone Ag Foam Dressing
- Alginate Dressing
- Silicone Postoperative Dressing
- Foam Dressing
- Medical Hydrogel Dressing
- Silicone Foam Dressing
- Silicone Foam Dressing Border Yoga
- Super Absorbent Dressing
- Gelling Fiber Dressing
- Collagen Wound Dressing
- Collagen Particles
- Silicone Tape
- Silicone Gel Scar Dressing
- Silicone Wound Contact Dressing
- Tech Services
Silver Sustained Release Antibacterial Technology

OptiSil Silicone Perforation Technology

Absorption and Degradation Metabolism Technology

Anti-adhesion Technology
- Blog
- Contact Us
- Case Study
Silver Alginate Dressing
Surgical Wound Upper Arm (Case 1)
21 yrs. old male with a surgical wound of the right upper arm status post amputation due to osteomyelitis. Patient medical history includes smoking and illicit drug abuse. Wound made remarkable progress during the (8) weeks of clinical trial. Wound bed granulated appropriately without any maceration and adhesion.

Surgical Wound Full Thickness-left Hip (Case 2)
82 yrs. old female with a non-healing surgical wound of the left hip associated with a hip replacement surgery completed approximately 14 months ago. Patient’s medical history included diabetes mellitus T-II, hypertension, hyperlipidemia, morbid obesity, and osteomyelitis. Due to rolled wound margins and significant tunneling plastic surgery evaluation was planned. Sharp debridement completed on the wound initially and after 7 weeks of dressing changes, improved granulation was noted and the patient was referred to a Plastic surgeon for the surgical closure. Wound was surgically closed and 100% wound closure was achieved within 8 weeks.
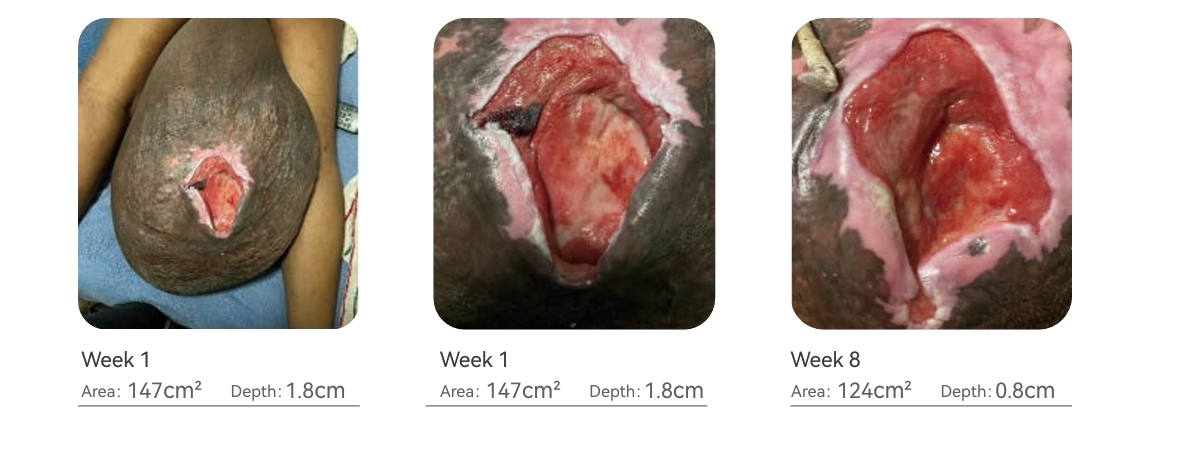
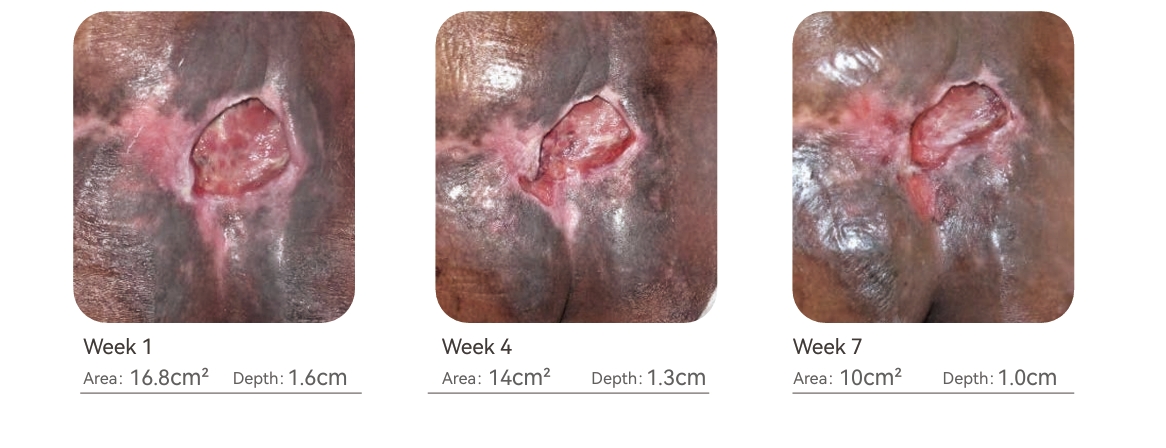
Stage IV Pressure Ulcer Scrotum (Case 3)
54 yrs. old male with a stage IV pressure ulcer of the Scrotum. Patient has enlarged scrotum due to the diagnosis of Hydrocele. Patient’s medical history includes hypertension, diabetes mellitus Type II and hyperlipidemia. Due to difficulty in off-loading of the affected area, complete wound closure was not achieved during the 8 weeks of treatment but increased granulation tissue and wound contraction was noted during the evaluation period. Moderate exudate was also well managed with the dressings.
Stage IV Pressure Ulcer Coccyx Region (Case 4)
66 yrs. old male with a stage IV pressure ulcer of the Coccyx region. Pressure injury caused tissue damage extended to the muscle with moderate drainage. Patient confined to bed acquired pressure ulcer due to bowel & bladder incontinence and lack of pressure relief. Patient’s medical history includes hypertension, hyperlipidemia, chronic kidney disease and malnutrition. Due to malnutrition and compliance issues wound closure was not achieved during the 8 weeks of treatment but significant improvement was noted during the evaluation period.distribution allowed the wound to make significant progress during the evaluation period.

Stage IV Pressure Ulcer Sacral Region (Case 5)
70 yrs. old female with a stage IV pressure ulcer of the Sacral region. Patient confined to bed acquired pressure ulcer due to bowel & bladder incontinence, bowel bladder incontinence, and malnutrition. Patient’s medical history includes congestive heart failure, hypertension, diabetes mellitus T-II, hyperlipidemia, chronic kidney disease and malnutrition. Wound had tissue damage extended to the muscle with tunnelingat 12 o clockand had copious serous drainage.Due to malnutrition and complex concurrent medical issues wound closure was not achieved during the 8 weeks of treatment but significant improvement was noted during the evaluation period.
Stage IV Pressure Ulcer Sacrum (Case 6)
68 yrs. old male with a stage IV pressure ulcer of the Sacrum. Patient s/p CVA with the right sided weakness and confined to bed acquired tissue injury due to incontinence and lack of off-loading. Patient’s medical history includes hypertension, diabetes mellitus Type II, hyperlipidemia and malnutrition. Due to malnutrition, elevated HgbA1c (9.5%) wound closure was not achieved during the 8 weeks of treatment but significant improvement was noted during the evaluation period. Full thickness wound with tissue damage was extended to the muscle and dressing changes with off loading and appropriate pressure distribution allowed the wound to make signifi cant progress during the evaluation period.

Stage IV Pressure Ulcer Sacro-coccyx Region (Case 7)
78 yrs. old female with a stage IV pressure ulcer of the sacro-coccyx region due to incontinence, bed confinement, malnutrition and advanced age. Pressure injury caused tissue damage extended to the muscle and bone with copious serous drainage and circumferential undermining. Patient medical history includes congestive heart failure, CVA, hypertension, and end stage renal disease. Wound made good progress during the (8) weeks of clinical trial. Wound bed was actively granulating and contracting but patient was hospitalized due to CHF exacerbation.
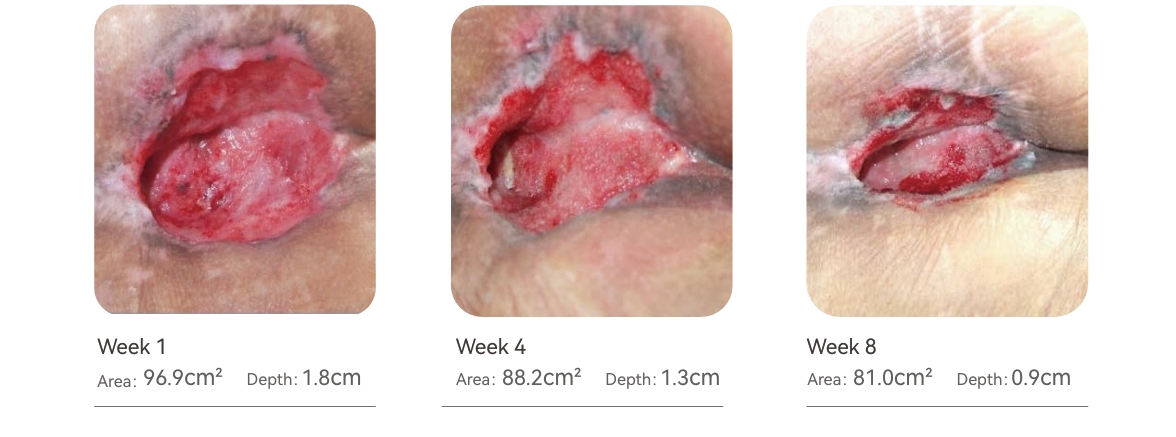
Stage IV Pressure Ulcer Left Hip (Case 8)
88 yrs. old female with a stage IV pressure ulcer of the left hip due to incontinence, bed confinement, malnutrition and end stage Alzheimer’s disease. Malnutrition and pressure injury caused tissue breakdown extended to the muscle and bone with copious sanguineous drainage and circumferential undermining. Patient medical history includes dementia, hypertension, and diabetes type II . Wound made significant progress during this evaluation period and showed positive effects of the dressing on the wound bed. Patient was on Hospice services.

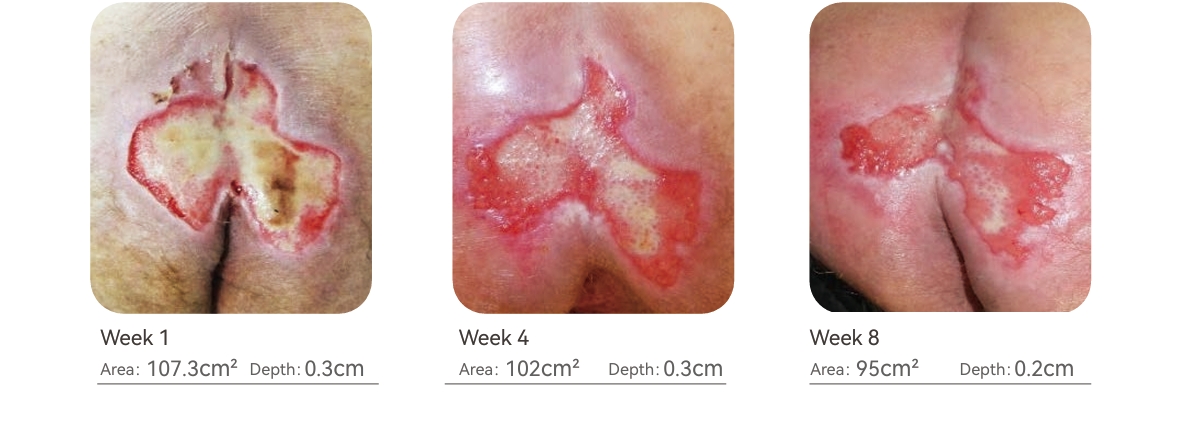
Stage III Pressure Ulcer Bilateral Buttocks (Case 9)
68 yrs. old female with a stage III pressure ulcer of bilateral buttocks. Pressure injury caused tissue damage extended to the subcutaneous tissue with copious serous-sanguineous drainage. Patient confined to bed acquired pressure ulcer due to bowel & bladder incontinence and malnutrition. Patient’s medical history includes smoking, coronary artery disease, hypertension, hyperlipidemia, and depression. Due to malnutrition and compliance issues wound closure was not achieved during the 8 weeks of treatment but significant improvement was noted. Dressing changes improved the wound bed and promoted active granulation.
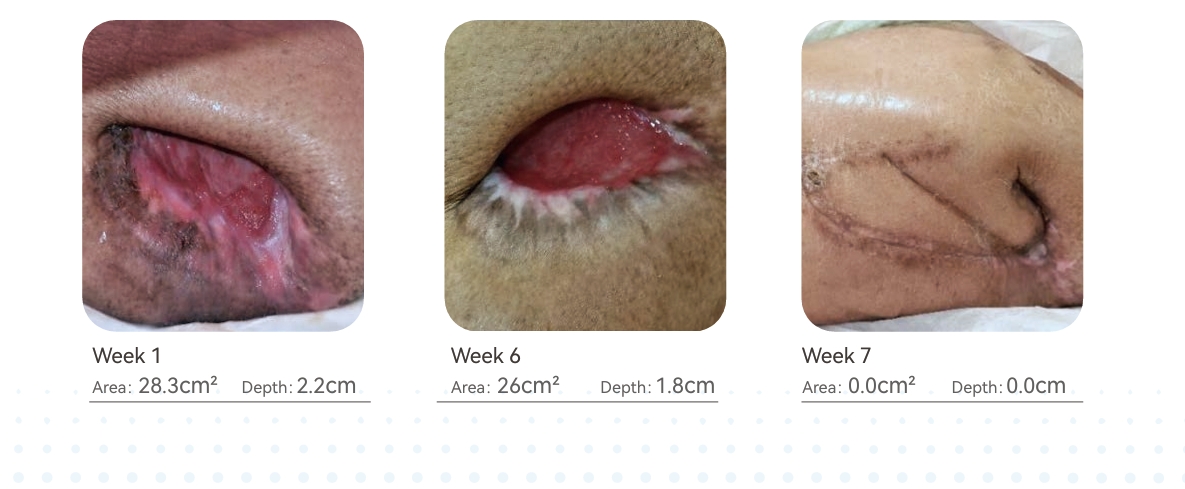
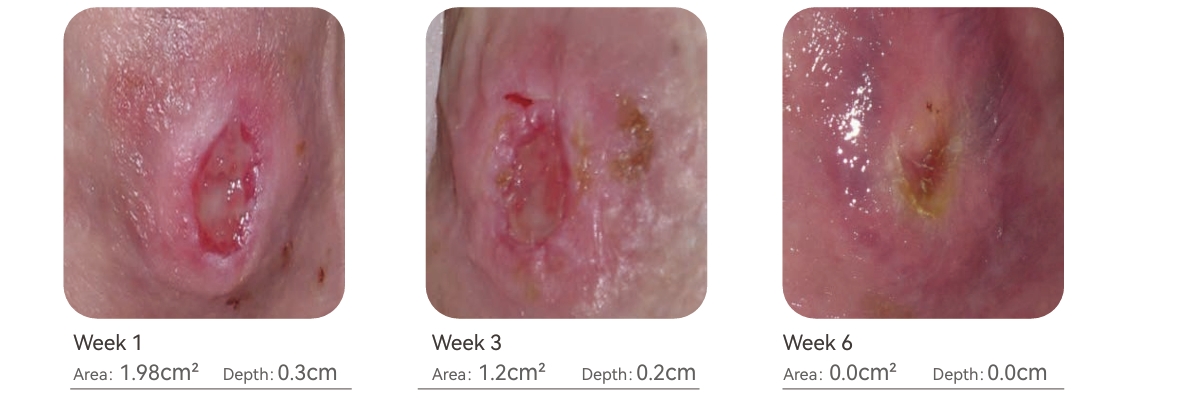
Stage III Pressure Ulcer Ankle (Case 10)
46 yrs. old female with a stage III pressure ulcer of the left ankle lateral aspect. Patient medical history includes; Multiple Sclerosis, bed confinement, generalized weakness, and hypothyroidism. During the (6) weeks treatment 100% wound closure was achieved. Off loading and dressing changes were effective in the timely closure of the wound.
Results
All (10) patients were evaluated weekly and wound surface area (cm2) & depth were carefully measured and recorded. In all (10) patients, wound contraction, tissue regeneration and bio-burden management were significant and no critical colonization was recorded. During the evaluation period all wounds showed improvement in size, drainage, and the percentage of granulation tissue present in the wound.
Discussion
This clinical case study was focused on maintaining a therapeutic environment during the proliferation phase of wound healing in full thickness wounds. In each clinical case, bio-burden of the wound was appropriately addressed initially through the culture & sensitivity testing and oral antibiotics. Application of Calcium Alginate with Silver (Ag) as a primary dressing in all clinical cases, was effective in maintaining wound bio-burden level and maintaining a moist wound environment ideal for regeneration of connective tissue. Critical colonization in wounds causes extended inflammation and thus delays the wound healing. Silicone foam was utilized as a secondary dressing in all clinical cases and found to be extremely effective due to its properties such as, protecting the wound base from external trauma, protecting the wound from external contamination, maintaining optimal vapor transfer rate and gaseous exchange necessary for cell metabolism, capability of absorbing exudate from the wound and preventing peri-wound skin maceration and conforming to the wound shape and size.
Conclusion
Based on our clinical evaluation results, it is concluded that Silicone foam dressing with adhesive borders and Calcium Alginate with Silver (LUOFUCON® ) were clinically effective in the management of full thickness wounds in any healthcare setting.
References
1. Mervis JS, Phillips TJ. Pressure ulcers: Pathophysiology, epidemiology, risk factors, and presentation. J Am Acad Dermatol. 2019;81(4):881–890.
2. Horn SD, Bender SA, Ferguson ML. The National Pressure Ulcer Long-term Care Study: pressure ulcer development in long-term care residents. J Am Geriatr
Soc. 2004;52:359–367.
Claim Your Free Sample Today
Discover how market-tested quality makes a difference. Request your free sample now and experience the superior performance of our wound dressings firsthand.




Visit Us
North Shangxia Rd. Dongjiang Hi-tech Industry Park, Huizhou, China
As a leader in advanced wound care, Foryou Medical specializes in innovative dressings, hemostatic products, and absorbable biomaterials. Since 2005, we’ve been dedicated to delivering high-quality solutions to meet global healthcare needs.
Showcasing Our Strengths






About Us
Copyright 2023, Hook BZOTech
